Secondary research:
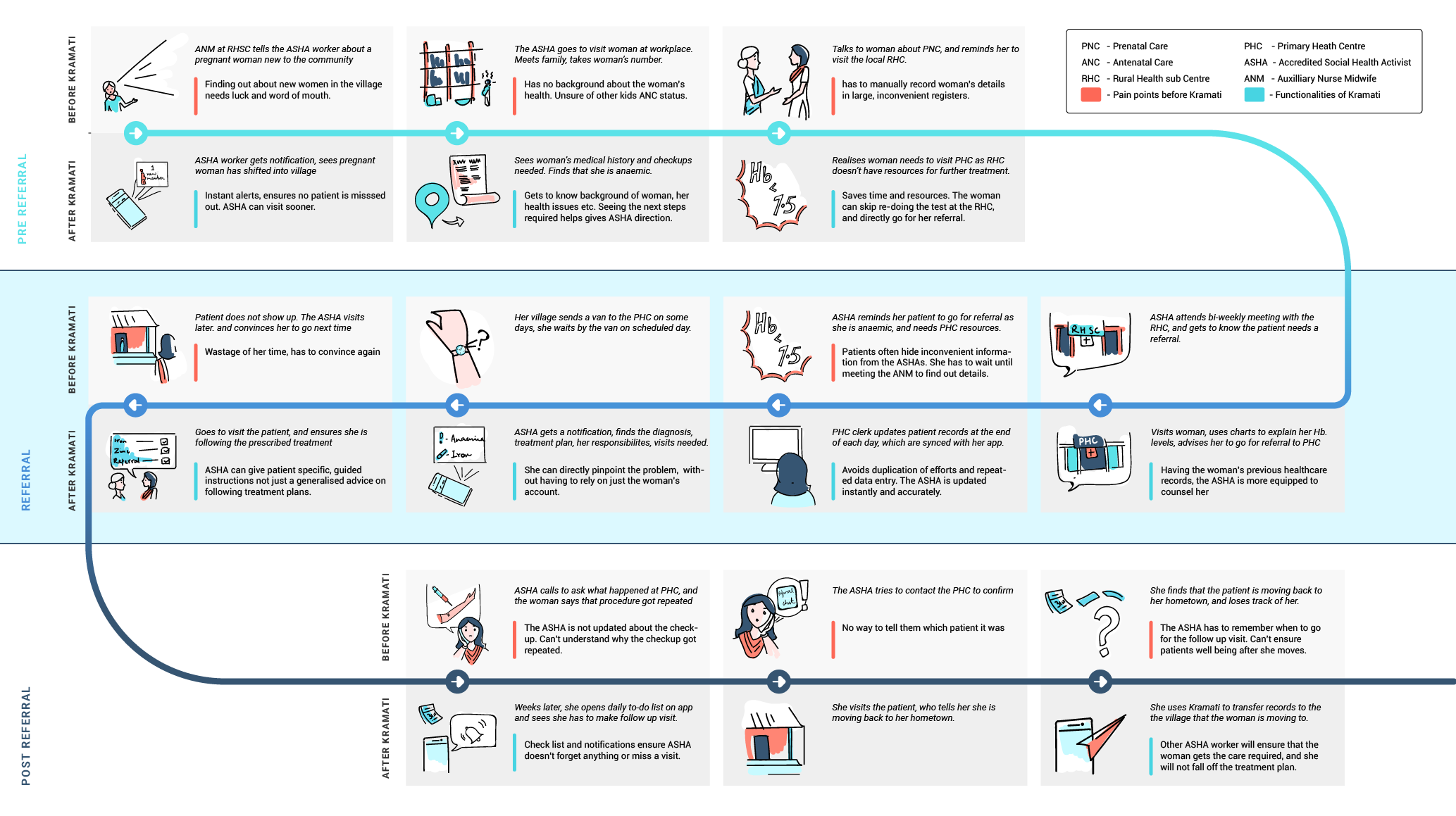
Besides doctors, India's rural healthcare system has several other workers, all with different levels of qualification and training.
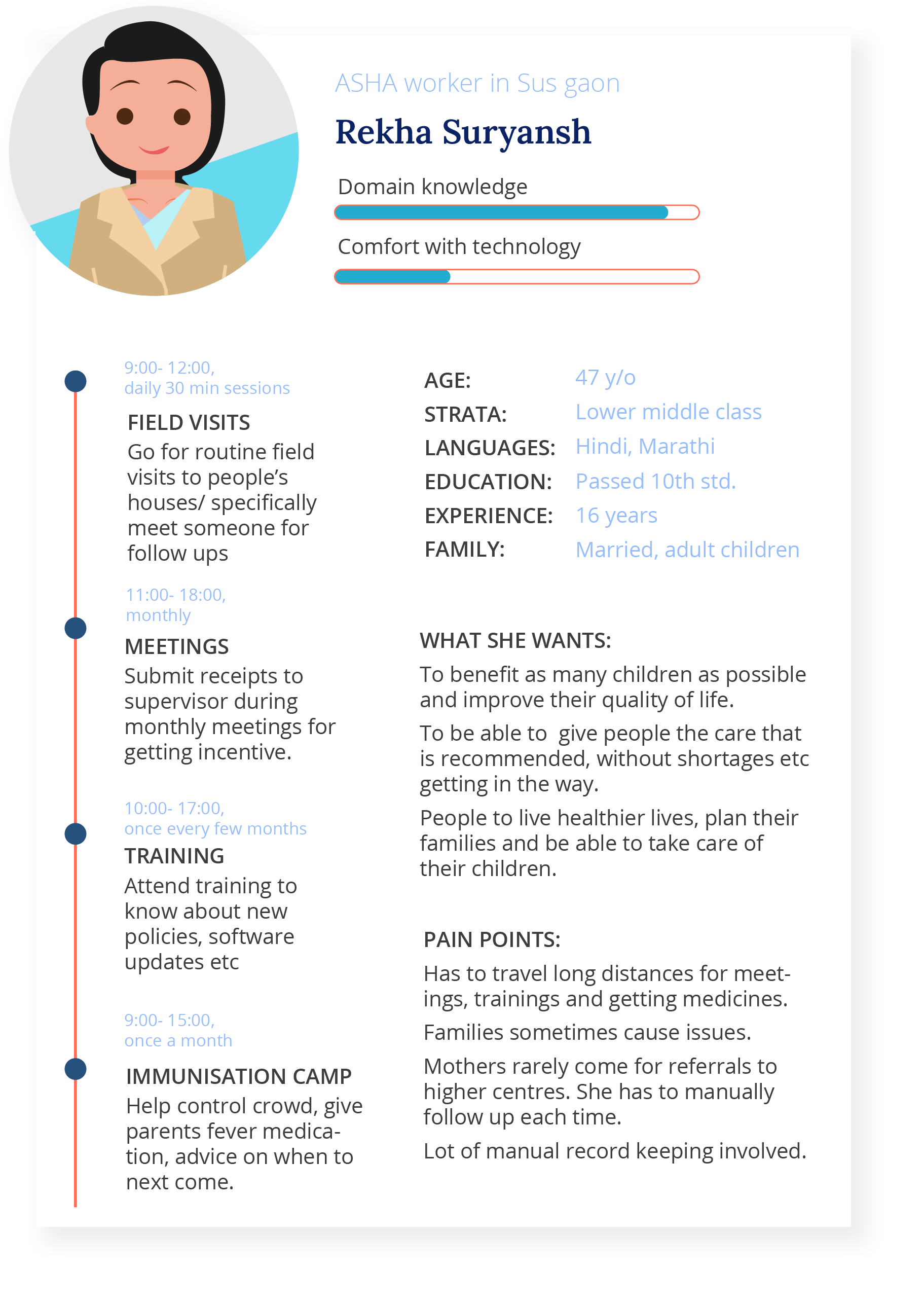
Accredited Social Health workers (ASHAs) visit homes to increase awareness of maternal health, sanitation, immunizations etc, help villagers access services, and provide basic medication, while Auxillary Nurse Midwives (ANMs) manage immunisations, prenatal and antenatal programs at primary health centers, and Anganwadi workers (AWWs) work in schools, focussing on childrens health.
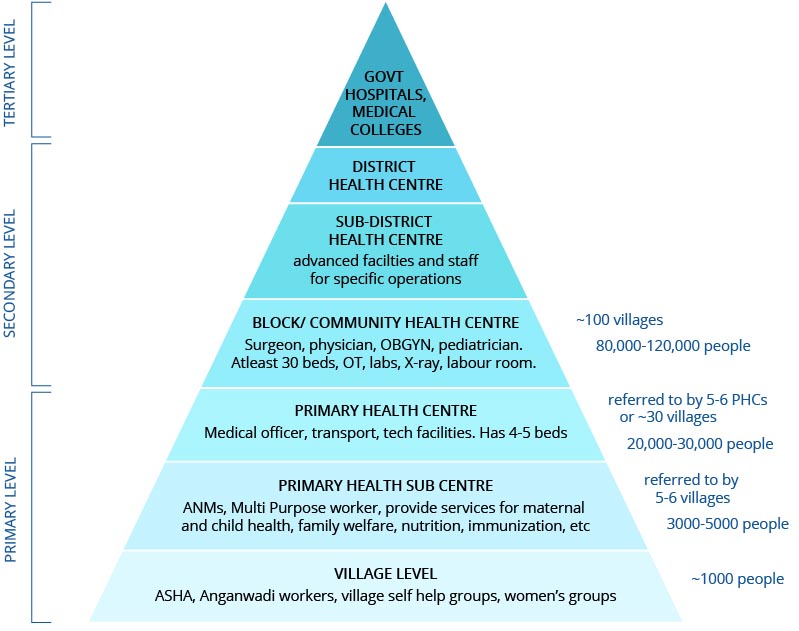
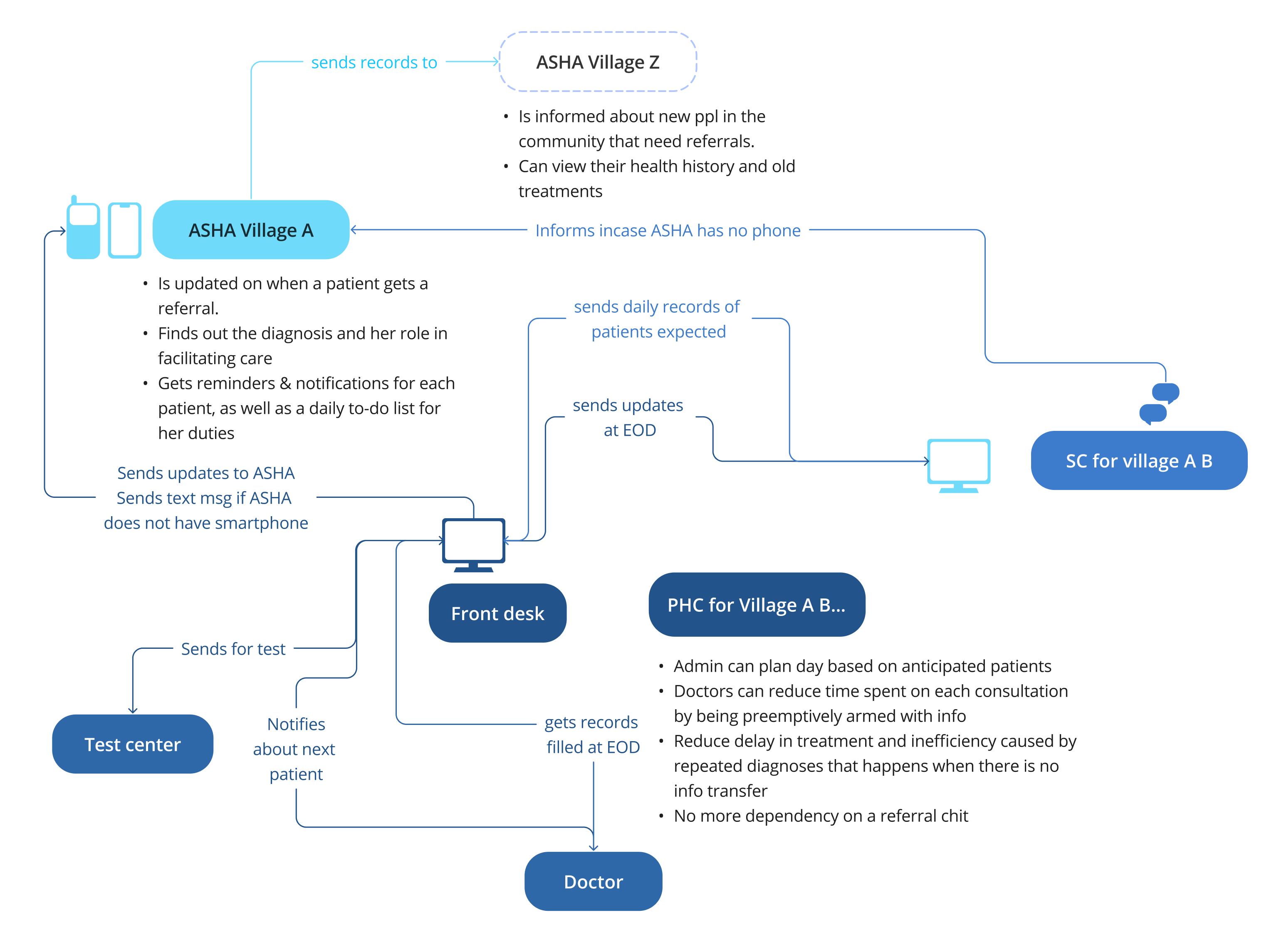
The rural healthcare system is tiered, as shown here. Each village has ASHAs and AWWs, every Sub Centre (SC) has an ANM, and each Public Health Centre (PHC) has a doctor. ASHAs and SCs refer patients to their PHC, and PHCs further refer upwards.